Most people think of diabetes medication as just a way to lower blood sugar. But for a huge group of people with type 2 diabetes, the real goal isn't just a better number on a glucose monitor-it's preventing a heart attack or kidney failure. This is where SGLT2 inhibitors is a class of oral medications that block the kidneys from reabsorbing glucose, forcing the body to flush excess sugar out through urine. Also known as gliflozins, these drugs have shifted from being a "last resort" option to a first-line defense for those with heart or kidney issues.
If you've been told you might start an SGLT2 inhibitor, you're probably wondering if the benefits for your heart outweigh the potential for side effects like yeast infections or the high cost of the pills. Here is a practical look at how these drugs work, who actually benefits from them, and the risks you need to discuss with your doctor.
Quick Summary: Key Takeaways
- Primary Goal: Lowers blood sugar and protects the heart and kidneys.
- Top Benefits: Significant reduction in heart failure hospitalizations and slower progression of chronic kidney disease.
- Common Risks: Genital yeast infections and urinary tract infections are the most frequent side effects.
- Critical Warning: Rare risk of euglycemic diabetic ketoacidosis (DKA), which can happen even if blood sugar levels seem normal.
- Best For: Patients with type 2 diabetes and existing cardiovascular or renal complications.
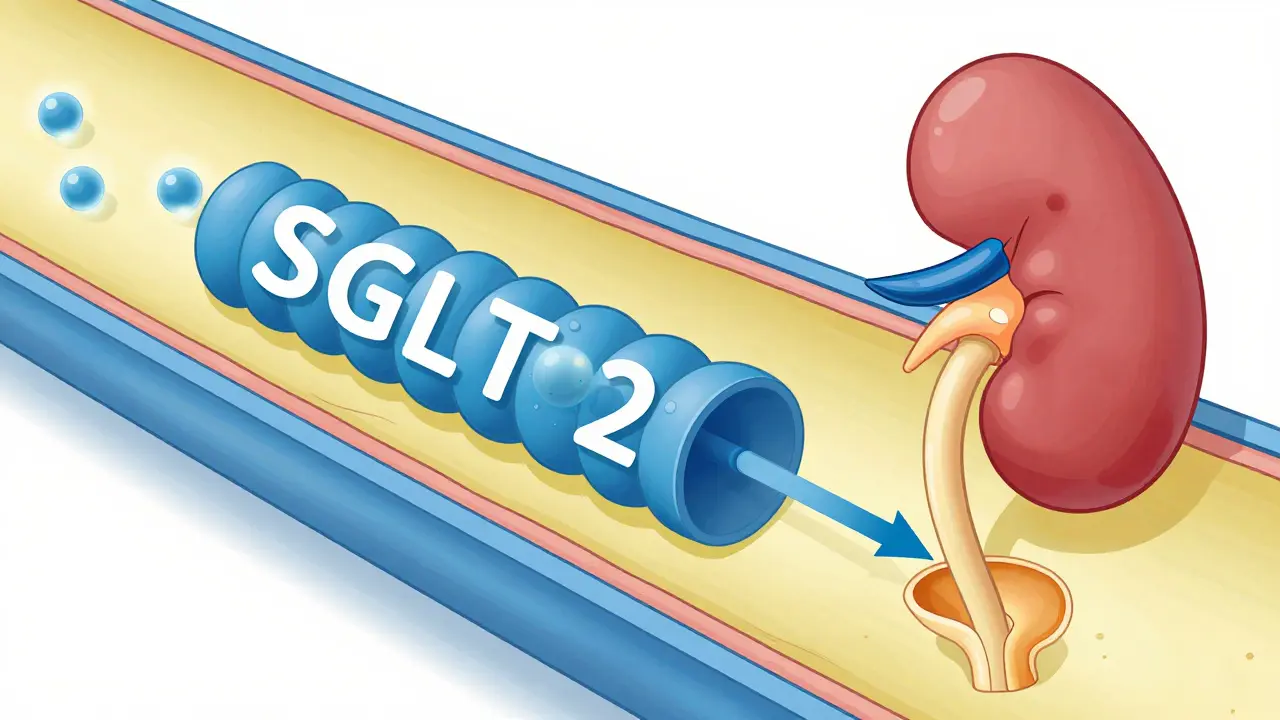
How SGLT2 Inhibitors Actually Work
Normally, your kidneys act like a filter that keeps the good stuff (like glucose) in your bloodstream and flushes the waste out. In people with diabetes, the kidneys often work too hard to pull that sugar back into the blood. SGLT2 inhibitors essentially "turn off" that reabsorption process in the proximal renal tubule. By blocking the sodium-glucose cotransporter 2 protein, these drugs force your body to pee out 40 to 100 grams of glucose every day.
Because you're dumping sugar, your HbA1c (your average blood sugar over three months) typically drops by 0.5% to 1.0%. But the real magic happens beyond the blood sugar. This process reduces the pressure inside the kidney's filters and helps the heart pump more efficiently, which is why these drugs are now prescribed even to some people who don't have diabetes but do have heart failure.
The Main Players: Comparing the Medications
There are four primary drugs in this class. While they all work similarly, they have different dosing and specific trial data backing them. For example, Empagliflozin (brand name Jardiance) is often praised for its strong heart-protective data, while Canagliflozin (Invokana) has shown impressive results in stopping kidney decline.
| Drug Name | Brand Name | Common Doses | Primary Strength |
|---|---|---|---|
| Empagliflozin | Jardiance | 10 mg, 25 mg | Strong reduction in cardiovascular death |
| Dapagliflozin | Farxiga | 5 mg, 10 mg | High efficacy for CKD regardless of diabetes status |
| Canagliflozin | Invokana | 100 mg, 300 mg | Significant reduction in end-stage kidney disease |
| Ertugliflozin | Steglatro | 5 mg, 15 mg | Effective glycemic control and weight loss |
The Big Wins: Heart and Kidney Protection
If you have heart failure, these drugs can be a game-changer. In trials like DAPA-HF, these medications reduced the need for hospital stays by about 30-35%. For many, this means the difference between staying home and spending a week in a hospital bed. One patient reported their ejection fraction-a measure of how well the heart pumps-improving from 28% to 42% after switching to a gliflozin.
Then there's the kidney factor. Chronic Kidney Disease (CKD) is a common and scary complication of diabetes. The CREDENCE trial showed that Canagliflozin could reduce the risk of reaching end-stage kidney failure by 30%. This isn't just about a lab value; it's about delaying or avoiding dialysis.
Beyond the heavy-duty protection, most users notice two "bonus" effects: weight loss and lower blood pressure. Since you're losing calories through your urine, it's common to drop 2 to 3 kilograms (about 4-6 pounds) early in treatment. Your systolic blood pressure also tends to dip by 3 to 5 mmHg, which takes additional stress off your arteries.
The Risks: What to Watch For
Nothing comes without a trade-off. Because you're putting more sugar in your urine, you're essentially creating a "sugar feast" for fungi and bacteria. This leads to the most common complaint: genital mycotic infections (yeast infections). Roughly 6% to 11% of users experience this. While annoying, it's usually manageable with good hygiene and over-the-counter treatments.
A more serious but rare concern is Euglycemic Diabetic Ketoacidosis (euDKA). Normally, ketoacidosis happens when blood sugar is sky-high. With SGLT2 inhibitors, your blood sugar might look perfectly normal, but your body starts producing ketones, which makes your blood acidic. This is a medical emergency. It's more likely to happen during a severe illness, a major surgery, or if you're fasting.
Finally, there's the risk of volume depletion. Because these drugs act as mild diuretics (making you pee more), older adults can get dehydrated. If you're already on a powerful blood pressure med or a diuretic, you might feel dizzy or faint. The FDA has even noted risks of acute kidney injury if you get too dehydrated too quickly.
Practical Guide: Starting and Maintaining Treatment
You shouldn't just jump into these medications without a plan. Because they rely on the kidneys to work, your doctor must check your eGFR (estimated glomerular filtration rate) first. If your eGFR is below 30, these drugs generally aren't started because they won't be effective at lowering glucose.
Here is a quick checklist for staying safe while on SGLT2 inhibitors:
- Stay Hydrated: Drink plenty of water to avoid dehydration and kidney stress.
- Prioritize Hygiene: Wash and dry the genital area thoroughly to prevent yeast infections.
- "Sick Day Rules": Talk to your doctor about whether to stop the medication temporarily during a severe illness or before surgery to avoid DKA.
- Monitor Feet: While rare, some reports suggest a risk of lower-limb issues; keep an eye on any unusual sores or swelling.
- Budget Plan: These drugs can be expensive (often over $600/month retail). Ask your pharmacist about patient assistance programs, which can drop the cost to $10-$25.
How They Compare to Other Diabetes Drugs
You might be weighing these against GLP-1 receptor agonists (like Ozempic or Mounjaro) or DPP-4 inhibitors. While GLP-1s are generally better for massive weight loss and preventing strokes, SGLT2 inhibitors are the clear winners for heart failure. In fact, they're much more effective at keeping you out of the hospital for heart issues than DPP-4 inhibitors.
The biggest advantage SGLT2 inhibitors have over older drugs like sulfonylureas is the lack of hypoglycemia. Since they don't force your pancreas to pump out insulin, you don't have to worry about your blood sugar crashing dangerously low while you sleep.
Can I take SGLT2 inhibitors if I have Type 1 diabetes?
Generally, no. These drugs are not approved for Type 1 diabetes because the risk of euglycemic diabetic ketoacidosis (euDKA) is significantly higher and much more dangerous in people who don't produce their own insulin.
Do these medications cause weight gain?
No, they actually cause weight loss. By flushing glucose (calories) through your urine, most patients lose between 2 and 3 kilograms in the early stages of treatment.
What should I do if I develop a yeast infection?
Genital infections are common. Start by improving daily hygiene and drinking more water. If symptoms persist, contact your doctor for an antifungal cream; most people can stay on the medication once they manage the infection.
Will these drugs work if my kidney function is very poor?
Their ability to lower blood sugar decreases as kidney function declines. Usually, if your eGFR is below 30, the drug is not recommended for glucose control, though some may still be used for heart failure protection under strict supervision.
Are there generic versions available yet?
Currently, no. The major brands like Jardiance and Farxiga are under patent protection. Generics are not expected to hit the market until roughly 2027 to 2029.
Next Steps and Troubleshooting
If you are a newly diagnosed patient, your first step is to get an eGFR blood test. If your results show kidney or heart stress, ask your doctor if a gliflozin is a better fit than a standard metformin-only approach.
For current users experiencing dizziness, check your other medications. You might be over-diurising. A simple adjustment in your blood pressure medication can often fix this without needing to stop the SGLT2 inhibitor.
If you are struggling with costs, don't just quit the med. Reach out to the manufacturer's patient assistance programs. Many patients who think they can't afford these drugs end up paying very little through these specific grants.