Itraconazole Dosage Calculator for Fungal Eye Infections
Fungal Eye Infection Dosage Calculator
Calculate the appropriate itraconazole dosing regimen based on your specific fungal pathogen type and infection severity. Note: This is for informational purposes only. Always follow your physician's guidance.
Important Information
Itraconazole dosing should always be determined by your healthcare provider based on culture results, drug sensitivity testing, and individual patient factors.
Important: Therapeutic drug monitoring (TDM) is recommended after 5 days of therapy to ensure serum levels stay between 1.0-2.0 µg/mL.
Recommended Dosage Regimen
Select your pathogen type and infection severity to view dosage recommendations.
When a fungal infection sneaks into the eye, vision can be at risk within days. Itraconazole is a systemic antifungal that many eye specialists turn to when topical options fall short. This guide walks you through when and how itraconazole is used for ocular fungal infections, the dosing strategies that work, safety checkpoints you shouldn’t miss, and what alternatives exist.
Understanding Fungal Eye Infections
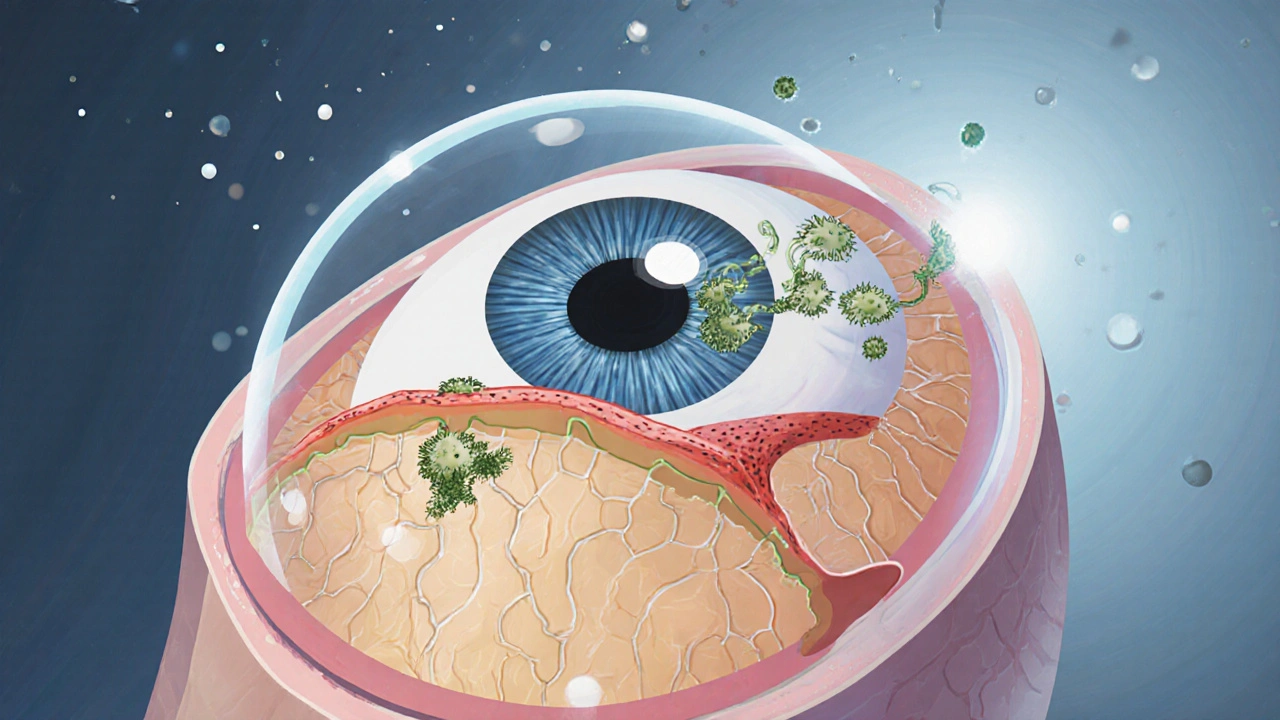
Fungal eye infections, often called fungal keratitis, occur when spores land on a compromised cornea - typically after trauma, contact‑lens wear, or chronic eye disease. The most common culprits are Aspergillus, Fusarium, and Candida. These organisms produce enzymes that dissolve corneal tissue, leading to ulceration, scarring, and sometimes permanent vision loss.
Because the eye has limited blood flow, many topical antifungals (like natamycin) can’t reach deep stromal layers. When the infection spreads beyond the surface, ophthalmologists often add an oral systemic agent - and itraconazole is a top choice for its broad spectrum and good ocular penetration.
How Itraconazole Works Against Eye Pathogens
Itraconazole inhibits the fungal enzyme lanosterol 14‑α‑demethylase, which is essential for ergosterol synthesis - the main building block of fungal cell membranes. Without ergosterol, the cell membrane becomes leaky and the fungus can’t survive. This mechanism works against a wide range of molds and yeasts, making itraconazole effective for the same organisms that cause keratitis.
Pharmacokinetic studies show that after a standard oral dose, itraconazole reaches a steady‑state concentration of about 2-5 µg/mL in the aqueous humor, which is within the inhibitory concentration (MIC) for most ocular fungi. That’s why clinicians consider it a reliable partner when the infection digs deeper than topical drops can reach.
When Do Doctors Choose Itraconazole?
- Deep stromal infection that doesn’t respond to natamycin or voriconazole eye drops.
- Infections caused by Aspergillus or Fusarium strains with known susceptibility to itraconazole.
- Patients who cannot tolerate voriconazole because of liver enzyme elevation or visual disturbances.
- Adjunct therapy after surgical debridement to prevent recurrence.
In each case, the decision hinges on laboratory culture results, drug‑sensitivity testing, and the physician’s assessment of how far the fungus has penetrated.
Dosage and Administration for Ocular Infections
The usual adult regimen for systemic fungal keratitis starts with a loading dose of 200 mg orally twice a day for the first 48 hours, followed by a maintenance dose of 200 mg once daily. For severe cases, some specialists extend the loading phase to 400 mg twice daily for the first three days, then reduce to 200 mg twice daily for a week before settling on 200 mg once daily.
Therapeutic drug monitoring (TDM) is recommended after five days of therapy to ensure serum levels stay between 1.0-2.0 µg/mL - the window that balances efficacy and toxicity. If levels fall short, the dose can be increased by 100 mg increments; if they exceed 2.5 µg/mL, the dose should be reduced or the drug paused.
Patients should take itraconazole with a full glass of water and a fatty meal, as food boosts absorption by up to 40 %. Splitting the dose (morning and night) can also help maintain steadier blood levels.
Monitoring Safety and Managing Side Effects
Most people tolerate itraconazole well, but eye‑related use calls for extra vigilance because systemic exposure is higher than in skin infections. Key safety checkpoints include:
- Liver function tests (LFTs) before starting, then weekly for the first month, and monthly thereafter.
- Serum electrolytes (especially potassium) if the patient is also on diuretics.
- Drug‑interaction review - itraconazole is a strong CYP3A4 inhibitor, so avoid concurrent use with statins, certain anti‑arrhythmics, and some HIV protease inhibitors.
- Visual changes - although rare, patients should report any new halos, flashing lights, or blurred vision immediately.
Common mild side effects are nausea, headache, and a metallic taste. If severe nausea persists, taking the drug with a light snack or switching to a liquid formulation can help.
Practical Tips for Patients on Itraconazole
- Keep a medication diary: note the time you take the dose, any meals, and side‑effects.
- Set a reminder on your phone for the twice‑daily loading phase; missing a dose can let the fungus rebound.
- Stay hydrated but avoid grapefruit juice, which can increase itraconazole blood levels dangerously.
- Plan follow‑up appointments every two weeks for the first month to review eye exam findings and blood work.
Adherence is crucial - studies show that patients who complete at least six weeks of therapy have a 90 % cure rate versus 55 % for those who stop early.

Alternatives When Itraconazole Isn’t Suitable
If a patient has severe liver disease, a known CYP3A4 interaction, or an infection caused by a fungus resistant to itraconazole, clinicians may turn to:
- Voriconazole - excellent ocular penetration but can cause visual hallucinations.
- Posaconazole - broader spectrum, but requires a loading dose and may be cost‑prohibitive.
- Amphotericin B eye drops - used for Candida keratitis when systemic therapy is contraindicated.
Each alternative comes with its own monitoring requirements, so the choice always balances efficacy, safety, and patient preferences.
Quick Reference: Common Ocular Fungi & Itraconazole Dosing
| Pathogen | Typical MIC (µg/mL) | Loading Dose | Maintenance Dose |
|---|---|---|---|
| Aspergillus fumigatus | 0.25‑0.5 | 200 mg BID × 2 days | 200 mg QD |
| Fusarium solani | 0.5‑1.0 | 400 mg BID × 3 days | 200 mg BID |
| Candida albicans | 0.12‑0.25 | 200 mg BID × 2 days | 200 mg QD |
| Fusarium oxysporum | 1.0‑2.0 | 400 mg BID × 3 days | 200 mg BID |
Adjust the maintenance dose based on serum levels and liver function, and always follow the ophthalmologist’s specific instructions.
Frequently Asked Questions
Can itraconazole be used as eye drops?
No. Itraconazole is not formulated for direct ocular use. It works systemically, reaching the eye through the bloodstream. For surface infections, clinicians prefer natamycin or voriconazole drops.
How long does treatment usually last?
Typical courses run 4-6 weeks, but may extend to 8 weeks if the ulcer is deep or if follow‑up exams show lingering inflammation.
Is itraconazole safe for pregnant women?
Itraconazole is classified as Pregnancy Category C. It should be avoided unless the benefits clearly outweigh the risks, and only under specialist supervision.
Do I need to get my blood tested while on itraconazole?
Yes. Baseline liver function tests are required, followed by weekly LFTs for the first month and periodic monitoring thereafter. Therapeutic drug monitoring is also advised after the first week to confirm adequate serum levels.
Can I take itraconazole with other medications?
Because itraconazole strongly inhibits CYP3A4, it can raise blood levels of many drugs, including certain statins, calcium channel blockers, and HIV protease inhibitors. Always provide your doctor a full medication list.
What should I do if I miss a dose?
Take the missed dose as soon as you remember if it’s within 12 hours; otherwise skip it and continue with the regular schedule. Doubling up can increase side‑effects and isn’t recommended.
Understanding how itraconazole works, when it’s indicated, and how to monitor its safety turns a scary eye infection into a manageable treatment plan. Talk with your ophthalmologist about whether this systemic antifungal fits your specific case.
Dan Danuts
October 23, 2025 AT 14:08Great overview of itraconazole-you’ve covered the essentials and then some!
When I first encountered a deep fungal keratitis case, the learning curve felt steep, but sticking to the dosing schedule made a huge difference.
The loading phase of 200 mg twice daily for two days really primes the system, and patients who actually take it with a fatty meal see noticeably higher ocular concentrations.
I’ve seen labs jump from sub‑therapeutic to within the 1.0‑2.0 µg/mL window after just a few days of proper adherence.
Because the drug is lipophilic, the timing with food isn’t just a nice suggestion-it’s a science‑backed requirement.
Remember to schedule liver function tests before you start, then weekly for the first month; catching a rise early spares the patient from serious hepatotoxicity.
If the LFTs creep up, a dose reduction to 100 mg BID often brings them back down without compromising efficacy.
Therapeutic drug monitoring after day 5 is a game‑changer, especially for those on concomitant CYP3A4 inhibitors.
In my practice, I also double‑check electrolytes when patients are on diuretics, because hypokalemia can exacerbate side‑effects.
Compliance is another big piece-set phone alarms, use pillboxes, and keep a simple diary.
Missing a dose during the loading phase can let the fungus rebound, so catching up within 12 hours is the safest route.
Patients often ask about grapefruit juice; the short answer is stay away, as it can push serum levels into dangerous territory.
Visual disturbances are rare, but any new halos or flashes should be reported immediately.
I’ve also found that counseling patients about the metallic taste upfront reduces anxiety and improves adherence.
When the infection responds, you can consider tapering to a maintenance dose of 200 mg once daily for the remainder of the 4‑6‑week course.
Overall, a disciplined approach to dosing, monitoring, and patient education turns a potentially blinding infection into a manageable condition.
Dante Russello
October 25, 2025 AT 01:53One thing worth noting, especially for clinicians who juggle multiple antifungal agents, is the nuanced safety profile of itraconazole, because it’s a strong CYP3A4 inhibitor, you’ll want to review the patient’s medication list carefully-statins, certain calcium channel blockers, and some HIV protease inhibitors can sky‑rocket in concentration, that said, when you compare it to voriconazole, itraconazole tends to have fewer visual side‑effects, which many patients appreciate, the dosing flexibility is also a plus; you can start with a loading phase and then step down to a once‑daily regimen without sacrificing ocular penetration, of course, regular liver enzymes are non‑negotiable, and you should schedule them weekly for the first month, then monthly thereafter, if the infection is caused by a Fusarium species with a higher MIC, consider augmenting therapy with an amphotericin B eye drop rather than switching agents outright, overall, the decision matrix balances efficacy, safety, cost, and patient preferences.
James Gray
October 26, 2025 AT 18:33Honestly, itraconazole is a real lifesaver for deep keratitis, and most docs definitely should consider it, the dosing schedule is simple, just follow the loading phase and then keep up with the daily dose, makin sure you take it with a fatty meal can boost absorption, it’s also pretty safe for most ppl, just keep an eye on liver tests, and if you feel nauseous, a light snack can help, overall it’s a solid option, definitely recomend it for those tough fungal eye infections.
Scott Ring
October 28, 2025 AT 12:13It’s helpful to remember that itraconazole’s systemic approach complements topical therapy nicely, especially when the infection has gone beyond the corneal surface, you’ll want to monitor liver enzymes regularly, and keep the patient informed about potential side‑effects like nausea or taste changes, staying proactive with appointments every two weeks can catch any issues early, and maintaining good communication ensures adherence.
Shubhi Sahni
October 29, 2025 AT 16:00I totally agree, the safety checks are crucial, especially the weekly LFTs, which help catch any hepatic issues early, also, the drug‑interaction review, is indispensable, because itraconazole can elevate levels of many co‑administered meds, and don’t forget the importance of a fatty meal, which really enhances absorption, finally, patient education, about timing and side‑effects, makes a huge difference.
Danielle St. Marie
October 30, 2025 AT 19:46While some may laud itraconazole as a "miracle drug," let’s not ignore the fact that its pharmacokinetics are far from trivial; only truly discerning clinicians appreciate the nuanced balance between efficacy and CYP3A4 inhibition, and, frankly, the over‑reliance on its broad‑spectrum claim can lead to complacency-let’s elevate the discourse, shall we? 🌟🤓
keerthi yeligay
October 31, 2025 AT 23:33Therapy length matters, 4‑6 wks is ideal.
Peter Richmond
November 2, 2025 AT 03:20In clinical practice, itraconazole remains a valuable adjunct for deep fungal keratitis, provided that hepatic monitoring and drug‑interaction assessments are routinely performed. The recommended loading dose, followed by a maintenance regimen, aligns with pharmacodynamic targets in ocular tissues. Patient compliance, supported by clear dosing instructions, is essential for therapeutic success.