Have you ever tried using a standard hearing aid only to find it doesn't help much when you have chronic ear infections or blockages? You are not alone. Many people struggle with traditional air-conduction devices simply because their specific type of hearing loss prevents sound from traveling normally through the ear canal. This is where Bone-Conduction Hearing Aids come in. Unlike regular aids that amplify sound waves into your ear, these devices send vibrations directly through your skull bones to the inner ear.
This alternative amplification method opens up communication for thousands of people who have been told they are "not candidates" for conventional devices. Whether you suffer from a blocked ear canal due to birth defects or have lost hearing in just one ear entirely, understanding this technology could change how you experience the world.
How Bone Conduction Technology Works
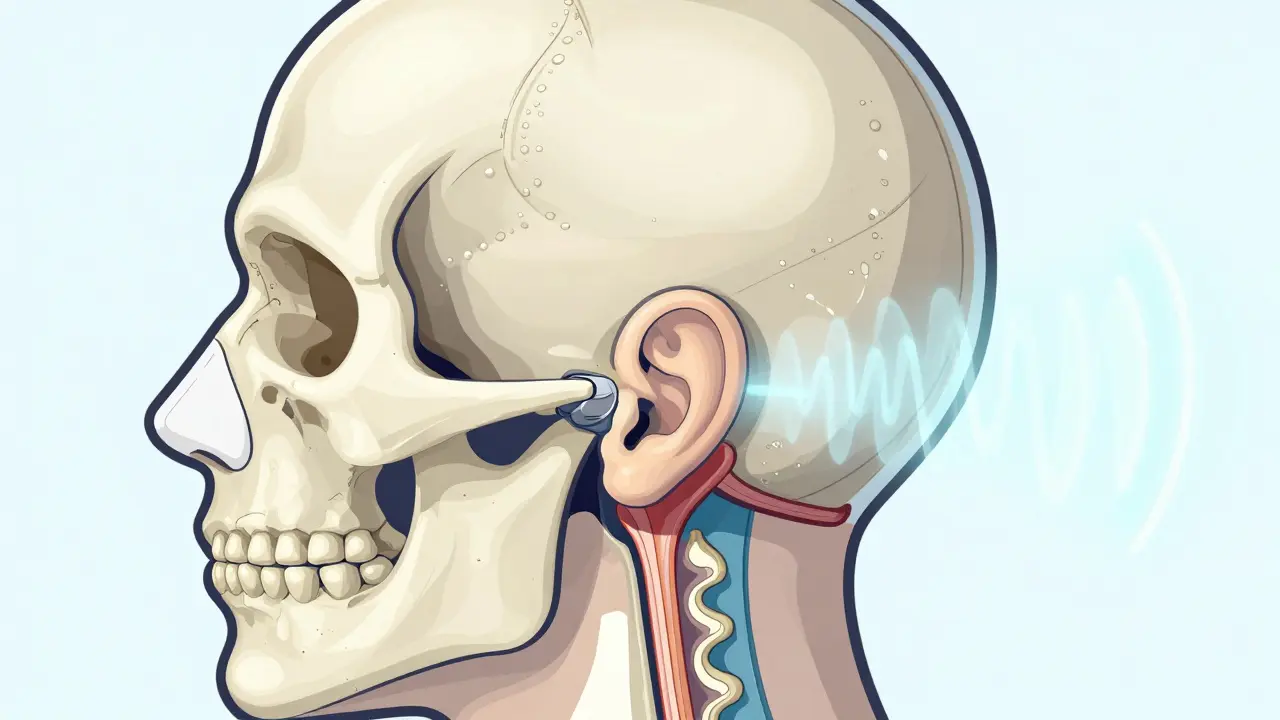
To understand why this helps, you need a basic picture of how hearing usually functions. Normally, sound waves enter your ear canal, vibrate the eardrum, and move tiny bones called ossicles before reaching the cochlea. The cochlea converts those vibrations into signals your brain understands.
Bone conduction bypasses the outer and middle ear structures entirely.When those first two stages break down-due to fluid, infection, or physical malformation-the signal never gets far enough along the line. A bone-conduction system skips that broken section completely. Instead of pushing air into your ear, a processor placed behind your ear creates mechanical vibrations. These travel through the temporal bone right to the cochlea.
Think of it like sending a message via mail versus courier. Standard hearing aids rely on the postal service (your ear canal) being open. Bone conduction hires a direct courier that delivers the package straight to your office (the inner ear). Research from Stenfelt and Goode highlights that cochlear fluid inertia accounts for about 60% of this hearing process, making it highly efficient even without the outer ear.
Who Is the Ideal Candidate?
Not everyone benefits from this technology. In fact, it is specifically designed for certain types of impairment. You should consider these devices if you fall into one of three primary groups.
First, people with conductive hearing loss. This occurs when sound cannot pass through the ear canal or middle ear. Common causes include chronic otitis media (persistent infections), where putting a standard aid in the ear traps bacteria and worsens the condition. Studies show that nearly 92% of patients with recurrent infections cannot use traditional aids safely. In these cases, bone conduction is the safer choice.
Second, individuals with congenital aural atresia. This is a birth defect where the ear canal fails to form. Success rates for fitting these patients hover around 85-90%, offering life-changing access to speech and environmental sounds they previously couldn't hear.
Third, those with Single-Sided Deafness (SSD). Approximately 9 million Americans suffer from total hearing loss in one ear while the other remains healthy. Traditional aids can't fix a dead inner ear, but they also can't route the quiet side's sound to the working ear effectively without causing confusion. Bone conduction helps by picking up sound on the deaf side and transferring it across the head to the working cochlea. User feedback suggests that 78% of SSD patients notice significant improvement in spatial awareness and localization after switching to this method.
Surgical Implants Versus Non-Surgical Options
You might assume you need major surgery for this, but there are two main paths forward. Knowing the difference helps you weigh the risks against convenience.
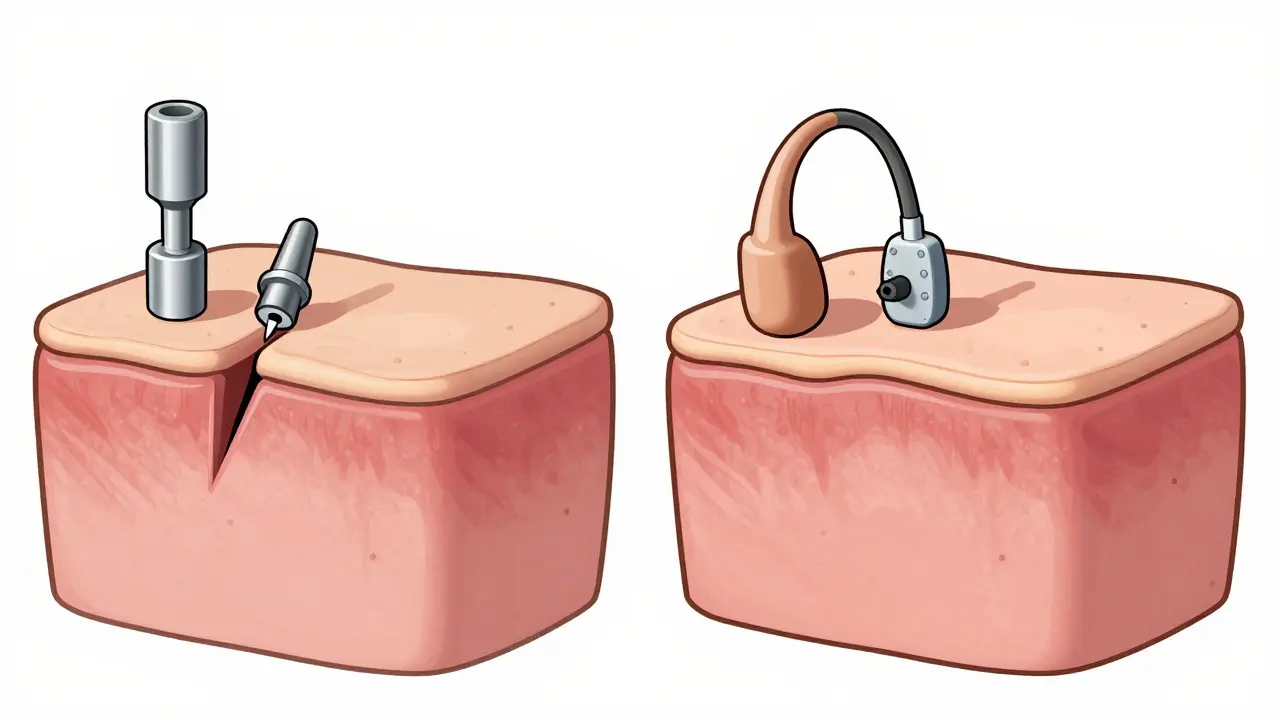
Percutaneous (Abutment) Systems
The classic example here is the BAHA Connect. This setup involves a minor outpatient procedure where a small titanium post is screwed into the skull bone. Your body fuses with this metal over 3 to 6 months, a biological process called osseointegration discovered by Dr. Per-Ingvar Brånemark decades ago. Once healed, the sound processor clicks onto the external abutment.
| Feature | Percutaneous (Abutment) | Transcutaneous (Magnetic) |
|---|---|---|
| Surgery Type | Titanium implant with protruding pin | Internal magnet under skin |
| Healing Time | 3-6 months for osseointegration | Immediate use (approx. 3 weeks recovery) |
| Maintenance | Daily cleaning of skin abutment | No daily skin hygiene needed |
| Signal Strength | Higher (less signal loss) | Slightly lower (skin attenuation) |
These percutaneous models generally offer stronger sound gain, making them ideal for severe conductive losses. However, you must keep the area clean. About 28% of users report some skin irritation around the post, requiring daily cleaning with alcohol wipes.
Transcutaneous (Magnetic) Systems
If you want to avoid poking holes in your skin, devices like the MED-EL Bonebridge or Cochlear BAHA Attract use magnets. During a brief surgery, surgeons place an internal magnet receiver under the skin, and the external processor snaps to it via magnetic force. Newer models often allow activation immediately after healing, though power transmission suffers slightly-usually 10 to 15 dB of loss-as vibrations must push through layers of tissue.
Surveys indicate that 92% of transcutaneous users are satisfied with the cosmetic look compared to 76% for visible abutments. For those sensitive to visibility or prone to skin infections, the magnetic option is often preferred despite the slight signal trade-off.
Cost Considerations and Insurance
Let's talk about the price tag, because bone conduction is significantly more expensive than a standard pair of hearing aids. In 2023, prices for implantable systems ranged from $4,000 to $7,000 per ear, whereas premium conventional aids often fell between $1,500 and $3,500. Keep in mind that costs have likely risen by 2026 due to market trends.
However, many insurance plans classify these devices differently because they often require surgery. The American Academy of Otolaryngology states that bone-anchored systems are medically necessary for patients who cannot benefit from conventional aids due to medical reasons. You should verify with your provider, but Level I evidence supporting efficacy has helped boost coverage approval rates over the last few years.
Also consider long-term maintenance. Batteries and processors need replacing every 3 to 5 years. While the implant lasts for decades, the external unit has a lifecycle cost similar to standard hearing aids, which helps balance the initial investment.
Living with a Bone Anchored Device
Adjusting to a new way of hearing takes practice. Most users adapt within two to four weeks, but there are quirks you should expect early on.
Sensation Changes: When you eat or chew with these devices on, you may hear your own jaw movement clearly. This "occlusion effect" is less of a problem than with traditional aids, but the sensation of vibration near the temple can take getting used to.
MRI Limitations: One major drawback to discuss before surgery is safety during scans. Metal implants generally mean you cannot undergo an MRI scan of 1.5 Tesla or higher without removing the internal components. If you anticipate needing frequent brain imaging, discuss this limitation with your neurologist beforehand.
Daily Care: If you choose the abutment style, hygiene is non-negotiable. Build a routine of cleaning the post once a day to prevent bacterial growth. If you get an infection, you might need revision surgery, which happens in about 8% of severe cases.

The Future of Bone Conduction
We are currently seeing rapid advancements in this niche. The latest iterations, such as the BAHA 6 Max, include Bluetooth 5.3 connectivity, allowing you to stream calls and music directly from your phone to the processor. Battery life has also improved, now lasting up to 30 hours on a single charge.
Furthermore, fully implantable systems are in development. Companies like Sonova are testing devices with no external parts remaining, aiming for FDA submission soon. These promise to eliminate the visual component entirely. Artificial intelligence is also coming to the processing chips, automatically adjusting background noise reduction in real-time-a feature expected to roll out widely in the next few years.
Frequently Asked Questions
Is the surgery for bone conduction hearing aids painful?
The procedure is typically performed under local anesthesia and takes 30 to 60 minutes. Most patients return to normal activities within 48 hours. Post-op swelling subsides in a week, though full integration takes longer.
Can I wear my bone conduction aid while swimming?
Generally, no. The external processors are water-resistant but not waterproof. You must remove them before submerging in water. Some newer models offer waterproof swim pods, but you still need to protect the implant site from prolonged exposure.
Will this help me if I have sensorineural hearing loss?
It depends on severity. Bone conduction is most effective for conductive loss. If your inner ear (cochlea) is damaged, gain is limited to about 45 dB. If your loss is beyond that threshold, a cochlear implant might be the better alternative.
Do children qualify for this technology?
Yes, children with congenital defects or recurring infections are often candidates. However, surgeons wait until age 4-5 for permanent implantation to ensure bone growth is stable, often starting with softband trial kits first.
How does bone conduction compare to CROS hearing aids?
CROS bridges signal between ears wirelessly. Bone conduction transmits physically through vibration. Studies show bone conduction provides better speech reception thresholds (15-20 dB advantage) and more natural sound localization for single-sided deafness compared to wireless CROS units.
Julian Soro
April 1, 2026 AT 14:46I had the abutment procedure back in 2021. The recovery was honestly smoother than anyone expected it to be. People worry about the skin infection risk around the post. You just have to maintain a strict hygiene schedule every single morning. My audiologist recommended alcohol wipes specifically designed for medical surfaces. The sound quality improved significantly once the osseointegration phase completed. You really notice the difference when you are in a noisy restaurant environment. Background noise reduction is much better compared to the traditional air conduction aids. I also experienced that strange feeling of vibration when I chewed gum initially. That sensation eventually fades into the background after about three weeks of use. Do not hesitate to contact your surgeon if swelling persists past the two week mark. Most patients return to normal activity levels very quickly after the appointment. Insurance coverage was surprisingly straightforward because of the medical necessity clause. Just remember that battery life depends heavily on streaming usage patterns throughout the day. Overall the investment pays off in quality of life improvements that you cannot measure.
Molly O'Donnell
April 1, 2026 AT 19:25I prefer the magnetic system simply because I dislike visible hardware on my head.
Russel Sarong
April 3, 2026 AT 11:51That is absolutely true!!! The cosmetic aspect is huge for social confidence!!!!! If you have to choose between performance and appearance, the transcutaneous option is way less obtrusive!!!!! It really changes how people react when you are talking in public places!!!!!
Eleanor Black
April 3, 2026 AT 18:19Indeed, the psychological impact of visibility is often overlooked in clinical discussions. Furthermore, one must consider the maintenance requirements regarding the skin site. Consequently, the choice between systems involves more than just technical specifications. Nevertheless, the percutaneous models do offer superior signal transmission fidelity. It is essential to weigh these factors carefully before proceeding. Additionally, the cost differential may play a significant role in decision making for many patients. We must prioritize the individual comfort of the patient above all else.
Callie Bartley
April 4, 2026 AT 15:23Everyone seems to forget about the insurance nightmare until it is too late. They tell you it is covered but then you get hit with denied claims anyway. I know someone who spent three months fighting the paperwork alone. The hospital billing department never picks up the phone on time either.
James DeZego
April 6, 2026 AT 03:51It can be frustrating 😔 but keeping all your receipts helps a lot 📝. Make sure to get pre-approval documentation signed before the surgery 📋. It saves so much headache later on 👍. Don't give up if the first claim gets rejected ❌.
Owen Barnes
April 6, 2026 AT 16:16I was worried about the MRI thing cos i might need scans someday. Does anyone know if the magent system works for fMRI or anything? Just trying to stay safe before gettin' the surgery done for real.
Rod Farren
April 7, 2026 AT 16:33Transcutaneous magnets generally interfere with high-field MRI protocols requiring removal or non-MRI conditional status verification. Modern devices utilize titanium alloys offering higher thermal stability during imaging sequences. However, artifact generation remains significant enough to obscure anatomical structures adjacent to the implant site. Consultation with neuro-radiology prior to procurement is mandatory for risk stratification.
Cara Duncan
April 9, 2026 AT 02:24This technology is amazing for families who struggle with communication daily 🎧. Seeing kids join their peers at school brings so much joy to parents ❤️. Please share your experiences if you have made the switch yourself 😊. We are all in this together supporting each other through the journey 🤗.
Christopher Beeson
April 10, 2026 AT 13:02Technology is merely a bandage for the inevitable decay of human biology. We seek to replace our natural functions with foreign objects. Is it worth surrendering autonomy to medical machinery for convenience? The soul of the body is compromised by such artificial augmentation.
Arun Kumar
April 11, 2026 AT 05:14While philosophy is important, practical solutions improve lives immensely for those suffering. Disability impacts dignity and connection with loved ones deeply. Helping others hear clearly restores a fundamental part of humanity. We should focus on reducing barriers rather than judging the tools used.
Jenny Gardner
April 13, 2026 AT 03:26The osseointegration period typically ranges between three and six months depending on bone density metrics. It is crucial to understand that individual healing rates vary significantly based on health conditions. Compliance with post-operative care instructions ensures optimal bonding strength for the abutment. Patients often underestimate the importance of patience during the initial fusion phase.
Rocky Pabillore
April 13, 2026 AT 06:49Most people lack the discipline required for proper abutment cleaning. Those who fail to maintain the site inevitably face revision surgeries. True understanding of the risks requires a sophisticated perspective that average consumers do not possess.
Cullen Zelenka
April 13, 2026 AT 12:19Looking forward to seeing AI features integrated into these processors soon. The market keeps innovating and helping more people connect with the world every year. Stay positive and keep researching your best options.