Living with ankylosing spondylitis (AS) means waking up every morning with stiffness that doesn’t fade with rest. It’s not just a bad back - it’s your spine slowly stiffening, your ribs struggling to expand, your posture changing without warning. For many, this starts before age 25, often mistaken for sports injuries or poor posture. But if your back pain lasts longer than three months, wakes you up between 3 and 6 a.m., and gets better when you move - not when you sit still - it’s likely more than just strain. This is ankylosing spondylitis, a chronic autoimmune disease that targets the spine and sacroiliac joints, turning inflammation into permanent structural damage if left unchecked.
What Happens Inside the Spine with AS
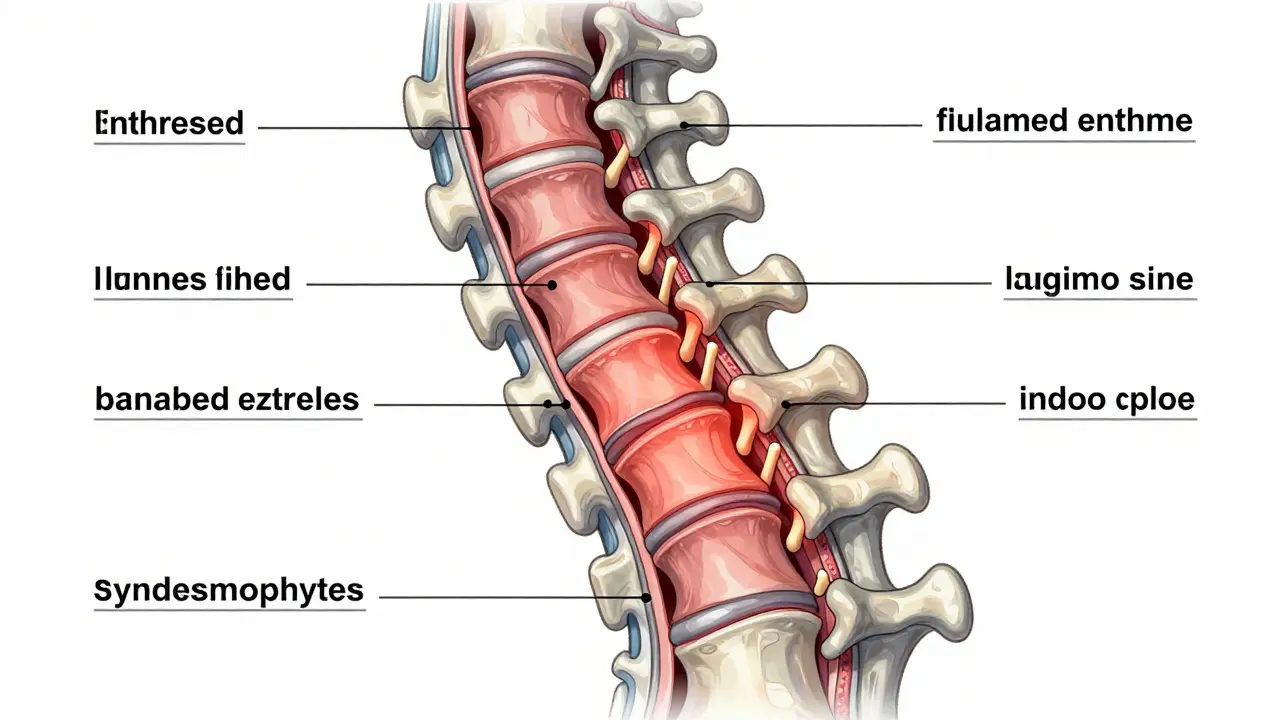
Ankylosing spondylitis doesn’t just hurt - it rebuilds. The body’s immune system attacks the entheses, the spots where tendons and ligaments connect to bone. In the spine, this leads to tiny fractures that heal with bone instead of tissue. Over time, these bony growths - called syndesmophytes - fuse vertebrae together. That’s why doctors call it “ankylosing,” meaning bony fusion. The result? A spine that looks like bamboo on an X-ray, with limited movement and increased fracture risk. About 90% of people with AS develop visible changes in their sacroiliac joints within ten years. Nearly half will have enough bone growth to limit spinal flexibility. And while not everyone ends up completely fused, the risk is real: 30-40% of untreated patients experience significant spinal fusion within 10 to 20 years. The disease is strongly linked to the HLA-B27 gene, found in up to 96% of Caucasian individuals with AS. But having the gene doesn’t guarantee disease - only about 5% of people with HLA-B27 actually develop AS. Genetics alone don’t tell the whole story.How AS Differs from Regular Back Pain
Most back pain comes from lifting, sitting too long, or a slipped disc. AS is different. It’s inflammatory. That means:- Pain lasts longer than 3 months
- Morning stiffness lasts more than 30 minutes
- Pain improves with movement, not rest
- Nocturnal pain that wakes you up
- Improvement after exercise, not after lying down
What Else Can AS Affect?
AS isn’t just about the spine. It’s a systemic disease. About one in three people with AS develop acute anterior uveitis - a sudden, painful eye inflammation that can lead to vision loss if untreated. Up to half may have inflammatory bowel disease (IBD), like Crohn’s or ulcerative colitis. Around 10% also develop psoriasis. These aren’t coincidences. They’re part of the same immune system overreaction. That’s why rheumatologists now group AS under the broader term “spondyloarthritis,” which includes related conditions like psoriatic arthritis and reactive arthritis. Fatigue is another major symptom, reported by 74% of patients as their most disabling issue. It’s not laziness - it’s inflammation in the brain and body. Many lose jobs, reduce hours, or quit careers because of it. Workplaces often don’t understand. One patient told me: “I used to be a mechanic. Now I can’t lift tools. They thought I was slacking. I had to prove I had a disease.”Medications: Stopping the Damage Before It Starts
NSAIDs like ibuprofen or naproxen are the first line of defense. They don’t just relieve pain - they slow down structural damage. Studies show that consistent NSAID use can cut radiographic progression by 50% over two years. But for many, that’s not enough. When NSAIDs fail, biologics step in. TNF inhibitors (like adalimumab or etanercept) and IL-17 inhibitors (like secukinumab) target the specific immune molecules driving inflammation. Clinical trials show 40-60% of patients achieve at least 40% symptom improvement within 12 weeks. Secukinumab, in particular, has been shown to reduce spinal bone growth by 55% over two years compared to standard care. In 2023, the FDA approved upadacitinib (Rinvoq), a JAK inhibitor, for active AS. It showed a 45% improvement rate at 14 weeks - nearly double the placebo rate. These drugs are powerful, but expensive. Without insurance, monthly costs range from $5,000 to $6,000. Insurance coverage has improved, but prior authorizations and step therapies still create delays. Some patients wait months before starting treatment.Mobility Strategies: Your Best Defense Against Fusion
Medication stops inflammation. But only movement can preserve function. The gold standard is daily physical therapy. Not once a week. Not when you feel like it. Every day. A structured program includes:- Spinal extension exercises (lying on your stomach, lifting your chest)
- Deep breathing to keep the rib cage flexible
- Shoulder rolls and chest openers to prevent forward hunching
- Aquatic therapy - swimming or water aerobics - which reduces joint stress
Posture and Daily Habits That Save Your Spine
How you sit, sleep, and stand matters more than you think.- Sleep on a firm mattress - no memory foam. Use a thin pillow or none at all.
- Sit with your back straight. Use a lumbar roll if your chair doesn’t support your lower spine.
- Stand with weight evenly distributed. Avoid leaning on one hip.
- Take breaks every 30 minutes if you sit for work. Walk, stretch, or do three spinal extensions.
Exercise During Flares: What to Do When It Hurts
You don’t have to push through pain. But you also can’t stop moving. During flares, switch to:- Heat therapy (heating pad or warm shower) for 20 minutes before exercise
- Gentle range-of-motion moves in bed - ankle circles, knee bends, shoulder rolls
- Water-based activities - even wading in a pool helps
- Short sessions: 10 minutes of movement, twice a day, instead of one long session
Why Community and Support Matter
AS is lonely. Most people don’t understand it. You can’t explain “bamboo spine” to your boss. You can’t show a photo of fused vertebrae to your friends. That’s why patient communities matter. The Spondylitis Association of America offers free online exercise videos watched by over 15,000 people monthly. MySpondylitisTeam has 8,000+ members sharing tips, medication reviews, and emotional support. One common thread? Those who joined a support group were twice as likely to stick with their exercise routine.What’s Coming Next
The future of AS care is faster diagnosis and smarter tools. MRI is now the preferred test for early detection - it finds inflammation before X-rays show bone changes. New drugs like JAK inhibitors are expanding options. Digital apps that track posture, pain, and movement are growing fast, with adoption expected to rise 30% annually through 2027. But the biggest breakthrough isn’t a drug. It’s awareness. The more people know - patients, doctors, employers - the earlier AS gets caught. And early action means a life with movement, not stiffness.Can ankylosing spondylitis be cured?
No, there is no cure for ankylosing spondylitis. But with early diagnosis and consistent treatment - including medication and daily exercise - most people can stop or significantly slow disease progression. Many live full, active lives without major disability. The goal isn’t elimination - it’s control.
Is ankylosing spondylitis genetic?
Yes, genetics play a strong role. The HLA-B27 gene is present in 88-96% of Caucasian AS patients. But having the gene doesn’t mean you’ll get the disease - only about 5% of people with HLA-B27 develop AS. Other factors, like infections or gut health, likely trigger the immune response in genetically susceptible people.
Can I still work with ankylosing spondylitis?
Absolutely. Many people with AS continue working full-time. Workplace accommodations - like standing desks, ergonomic chairs, flexible hours, or remote work - help significantly. Under the Americans with Disabilities Act (ADA), employers must provide reasonable adjustments. The key is communicating your needs early and using tools like posture reminders or short stretch breaks.
What’s the best exercise for ankylosing spondylitis?
The best exercise is the one you do consistently. Swimming, walking, yoga designed for AS, and tai chi are all excellent. Focus on spinal extension, deep breathing, and flexibility. Avoid high-impact sports like running or contact sports that risk spinal injury. A physical therapist specializing in AS can create a personalized routine. Studies show daily 30-45 minute sessions improve mobility by 25-30% in six months.
Do I need to take medication forever?
For most people, yes. AS is a lifelong condition. Stopping medication often leads to flare-ups and increased joint damage. Some patients who achieve long-term remission may reduce doses under doctor supervision, but complete discontinuation is rare. The goal is to find the lowest effective dose that keeps inflammation under control - not to stop treatment entirely.
Nandini Wagh
February 27, 2026 AT 07:54Wow. I read this while sipping chai at 3 a.m. because my spine decided to host a rave in my lower back. Seriously though - this is the first time someone explained AS like it’s not just ‘bad posture’ or ‘you’re getting old.’
Also, ‘bamboo spine’? That’s either a metal band name or a horror movie plot. Either way, I’m claiming it.
And yes - I quit yoga after two weeks because ‘stretching’ felt like being slowly turned into a human paperclip. Then I tried swimming. Now I cry happy tears when I can touch my toes. No joke.
Lillian Knezek
February 28, 2026 AT 19:40They’re lying. AS isn’t autoimmune. It’s a bioweapon. The HLA-B27 gene? That’s not natural - it was engineered in a lab to target people who sleep on memory foam. I’ve seen the documents. The CDC’s been covering it up since 2012. They want us stiff so we can’t protest. 😈
Also - your MRI? They inject nanobots. That’s why your spine ‘lights up.’ They’re mapping you. Wake up.
tia novialiswati
March 2, 2026 AT 15:01OMG YES. 😭 I’ve been living with this for 8 years and no one gets it. I just started swimming 3x a week and my morning stiffness went from 2 hours to 20 minutes. I’m crying right now. You’re not alone. I’ve got your back. 🙌
Also - if you’re using a lumbar roll, please tell me your brand. I need a new one and I’m too tired to research it again. I’ll send you cookies. 🍪
Stephen Archbold
March 2, 2026 AT 20:37Man, I read this after my physio session. I’ve been doing the spinal extensions every morning since last April. Still can’t touch my toes, but I can now pick up my cat without groaning. That’s a win.
Also - water aerobics changed my life. I swear, if I hadn’t found the local Y’s AS class, I’d be on disability by now. Don’t quit. Just move. Even if it’s slow. Even if it hurts. Just move.
Nerina Devi
March 3, 2026 AT 09:47I’m from India. AS here is invisible. Doctors say ‘it’s just aging.’ My aunt was told she’s ‘too emotional.’ I’ve been doing daily stretches since I was 22. No meds. Just yoga, walking, and refusing to let anyone call it ‘laziness.’
One thing they don’t say: the silence hurts more than the pain. Thank you for saying this out loud.
Christina VanOsdol
March 4, 2026 AT 15:32Okay, let’s unpack this. NSAIDs cut progression by 50%? That’s a 1-in-2 chance? That’s not ‘treatment’ - that’s a coin flip. And biologics? $6,000/month?! That’s not healthcare - that’s extortion. And JAK inhibitors? They’re just repackaged immunosuppressants with a new logo.
Also - ‘daily exercise’? Who has time? You work? You have kids? You pay rent? You’re telling me to swim 45 minutes a day while my insurance denies my prescription? This is a survival guide for the privileged.
And don’t get me started on ‘community support.’ My Facebook group has 3,000 members. 2,900 are just posting memes. 90 are asking for help. 1 responds. That’s not community. That’s noise.
Joanna Reyes
March 5, 2026 AT 10:44I’ve been on secukinumab for 18 months. I was skeptical. I thought it was just another expensive placebo. But after the third month, I could turn my head to look over my shoulder without pain. I cried. I didn’t even know I’d forgotten what that felt like.
Also - the fatigue? It’s not mental. It’s cellular. It’s like your body’s running a 100-mile race every day. And no, coffee doesn’t fix it. Sleep doesn’t fix it. Only treatment does.
And yes - I use a standing desk. I also have a heating pad permanently plugged in under my chair. I’ve accepted that my life is now a medical device commercial. But I’m alive. And I’m moving. That’s enough.
Christopher Brown
March 5, 2026 AT 17:20Why are we treating this like a yoga problem? This is a weakness. Weak bodies get weak spines. Weak people don’t lift. Weak people don’t move. You want to fix this? Lift heavy. Run. Get tough. Stop whining about water aerobics.
Also - HLA-B27? That’s a white person gene. You think this is common in Asia? No. It’s a Western disease. Stop medicalizing normal aging.
Ashley Johnson
March 6, 2026 AT 10:36Wait - you’re telling me this is an autoimmune disease? But I read online that AS is caused by 5G towers. The government uses it to track people who don’t wear masks. Also - the ‘bamboo spine’ is actually a secret government implant. They put it in during flu shots. I’ve got the X-rays. I’ll send them.
And the meds? They’re laced with microchips. That’s why you feel worse at first. Your body’s rejecting the tracker. You need to stop all meds. Eat raw garlic. Sleep on a bed of magnets. I did it. I’m walking again. No drugs. Just faith and zinc.
Maranda Najar
March 7, 2026 AT 21:59I’ve been living with AS since I was 19. I’ve lost jobs. I’ve lost friends. I’ve lost the ability to hug my niece without wincing.
But tonight - after 11 years of silence - I read this and I sobbed. Not because I’m broken. Because for the first time, someone didn’t say ‘just stretch more.’ They said: ‘This is real. This is systemic. This is not your fault.’
They didn’t say ‘you’re lucky.’ They didn’t say ‘at least it’s not cancer.’ They said: ‘This is a disease. And you deserve to live.’
I’m not fixed. But I’m seen. And that? That’s everything.
Dinesh Dawn
March 8, 2026 AT 11:31My dad had this. He didn’t know. Thought it was ‘just old age.’ Died at 58. Spine was completely fused. No one told him to move. No one told him to swim.
I’m 27. I do my stretches. I use the app. I don’t skip. Not because I’m strong. Because I don’t want to be him.
Nandini Wagh
March 9, 2026 AT 04:10And now I’m replying to myself because I’m that person. The one who still does 10 minutes of spine extensions while watching Netflix. The one who has a heating pad taped to her chair at work. The one who still gets weird looks when she asks for a standing desk.
But I’m here. And I’m moving.
So are you.